
Soon after she received the treatment, Karen Koehler’s brain swelled. Her blood pressure plummeted. As she fell into a coma, her husband and sister sat at her bedside — urging the doctors to keep pushing her farther along the razor’s edge between life and death.
Koehler was undergoing a promising — and terrifying — experimental therapy that her oncologists hoped could rid her body of cancer entirely. It’s called CAR-T therapy, and it works by engineering the patient’s own immune cells to attack cancer.
One of the hallmarks of CAR-T: It has to nearly kill you if it’s going to save you. The treatment induces such sudden and severe side effects that it can take a small army of top specialists to keep patients alive while their newly engineered immune systems attack their cancer cells.
The result: CAR-T remains so risky, so complex, and so difficult to manage that experts warn it’ll be years before it’s available to most patients who would stand to benefit — even though two drug makers, Novartis AG and startup Kite Pharma Inc., are racing to get their versions of the therapy approved by regulators as early as next year.
“The thing is, cellular therapies are extraordinarily complex drugs,’’ said Dr. Michael Milone, a CAR-T scientist at University of Pennsylvania.
CAR-T has been tested on hundreds of patients, mostly with blood cancers; solid tumors pose more of a challenge. Proponents say it’s just about ready for prime time. But it’s still quite early, cautions Bruce Levine, a gene therapy professor at University of Pennsylvania. (Both Levine and Milone are working with Novartis on its CAR-T therapy.)
“We’re in the Model T phase,’’ Levine said.
An infusion of Frankenstein cells
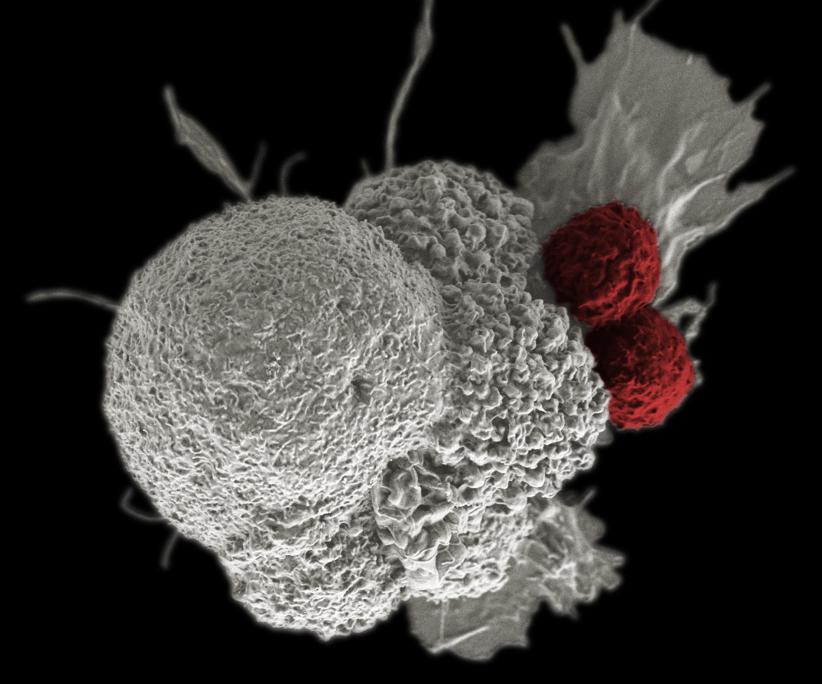
CAR-T therapy, short for chimeric antigen receptor T cell therapy, works like this: Physicians draw a patient’s blood and harvest her cytotoxic T cells — that is, cells that are already circulating in her body and are designed to attack infected or malignant cells.
The cells are reengineered in a lab so they can learn how to attack her particular cancer. The patient is then usually treated with chemotherapy to wipe out some of her existing immune cells, to give the engineered ones more room to replicate.
The therapy itself consists of an infusion, with the Frankensteinian T cells are fed back into the patient’s bloodstream, where they proliferate and work furiously to kill tumor cells. A single T cell can wipe out up to 100,000 cells.
But here’s the rub: Adding hyperactive T cells can cause the body’s immune response to go haywire.
Patients often wind up with a condition called cytokine release syndrome, which occurs when T cells excrete huge quantities of cytokines — small proteins involved in cell signaling. A “cytokine storm’’ can cause severe fevers, nausea, extreme fatigue, difficulty breathing, low blood pressure, and organ swelling.
In other words, it feels like the worst imaginable case of flu — which, of course, can be devastating in a patient already weakened by cancer and chemotherapy.
“The more tumor you have in your body, the more severe the cytokine release syndrome,’’ Milone said. As the tumors go away, the cytokines go away, and symptoms subside. A number of rudimentary tools are being used to temper the side effects of a CAR-T infusion, including steroids and drugs more typically used to treat juvenile arthritis.
But few physicians have a grip on how to appropriately treat cytokine release syndrome, because it’s so rare in everyday practice, Milone said.
A second complication associated with some CAR-T therapies is neurotoxicity: Patients often experience memory loss, hallucinations, and swelling of the brain. Researchers still don’t know much about what causes the neurotoxicity, but it’s already proven deadly.
Last month, three patients with acute lymphoblastic leukemia enrolled in a Juno Therapeutics Inc. CAR-T clinical trial died from complications including neurotoxicity, prompting the Food and Drug Administration to temporarily halt the trial.
Juno attributed the deaths in part to one of the chemotherapy drugs, fludarabine, given to patients before they received their infusion of engineered cells.
After Juno rewrote the trial protocol to eliminate that drug, the FDA allowed it to restart.
“I think we have made significant progress with cytokine release syndrome,’’ said Steve Harr, chief financial officer of Juno Therapeutics. “But we have a lot more to do with neurotoxicity.’’
Juno now hopes to get its drugs approved as early as 2018.
On their own, cytokine storms and neurotoxicity are both highly dangerous. Karen Koehler was hit with both.
When vomiting is good news
A teacher and golfer who lives in New Jersey, Koehler was diagnosed with chronic lymphocytic leukemia in 2011. It’s a form of blood cancer that’s often fairly benign, and for the first few years, doctors advised her to simply keep checking in.
“I felt healthy, but doctors basically told me I had this nuclear bomb in my body,’’ said Koehler, 59. “I just didn’t know if or when it would go off.’’
Still, she carried on, even naming her blood cancer “Lucy and Ethel,’’ which has the letters “CLL’’ in it. But in 2014, her cancer suddenly changed, from seemingly innocuous to terminal. She was told that chemotherapy wouldn’t work in her case, and was given a maximum of two years to live.
Stunned, Koehler began looking for options. A physician told her that an experimental therapy called CAR-T was working wonders for other patients with her specific cancer, and she enrolled in a trial at Memorial Sloan Kettering Hospital in New York.
Engineering the cells to infuse them back into the patient can take from a few days to a few weeks. In Koehler’s case, her blood was drawn in October 2014, and she didn’t receive the therapy until February 2015.
She was fitted with a catheter under her arm on a Friday. On Saturday and Sunday, she was given chemotherapy — a combination of the drugs fludarabine and cytoxan. Koehler didn’t have any reaction at that point.
“The big joke through all of this was how good I looked,’’ she said. “My husband is bald, so I can’t tell you how many times I was sitting in hospital, and doctors would start talking to him, instead, because he was bald.’’
On Tuesday, she got her “bag of cells’’ infused. It was no big deal. She sat, chatting, as nurses bustled in and out to check her vitals.
An hour later, she started getting sick. It was a sign that her immune system was kicking into overdrive.
“When I started throwing up, I thought, ‘Oh my god, this is great,’ ’’ Koehler said. Then, it wasn’t. Her heart started beating erratically. Her blood pressure dropped. Then brain swelling. Delirium. A coma.
They moved her to the intensive care unit. And that’s where she stayed, for eight days.
Her husband and her sister, a nurse, told the doctor to “take her as far as you can take her,’’ Koehler said. They didn’t want to stop the process prematurely, and risk not killing all of the cancer.
“But I got to the brink, and they said enough,’’ Koehler said. Doctors gave her an infusion of steroids, which shuts down the T cells that cause the cytokine storm — and also halts their aggressive attack on the cancer.
When she came to, Koehler just remembers being confused. Thanks, most likely, to the effects of the fludarabine, she had frequent, severe hallucinations. She imagined the nurses were selling blood next door. That she was on a TV show about golf.
“That stuff was scary — I knew the hallucinations were just a bad dream, but they seemed so real,’’ she said.
Koehler was in the hospital for three weeks. Her costs were covered by insurance and by Juno, since she was part of their clinical trial. But the costs for treating future patients could be enormous, with potential bills running hundreds of thousands of dollars.
Harr, the CFO of Juno has seen estimates as high as $500,000 to $750,000 — though said that doesn’t necessarily reflect how Juno will price its own CAR-T therapy.
Koehler’s hallucinations persisted for several weeks after she left the hospital, as did the confusion. But the treatment worked. By March 28, she was able to make it down to Florida for a family reunion. She golfed nine holes.
A ‘suicide switch’ to turn off therapy
Koehler’s experience shows just how tantalizing CAR-T is: A year and a half after the treatment, she remains free of cancer.
Dr. Stephanie Goff, a surgeon at the National Cancer Institute who’s working with Kite on its treatments, said CAR-T seems to work in about half of patients with lymphomas and leukemias who have run out of other treatment options, though some studies suggest the response rate is higher in certain patient populations, such as children with acute lymphoblastic leukemia.
But the side effects Koehler experienced, and the enormous amount of expertise it took to manage them, illustrate the risks of expanding the therapy to a broad patient population. So far, it’s been tested in just a handful of academic hospitals, including the University of Pennsylvania and Memorial Sloan Kettering in New York.
To bring CAR-T mainstream, biotech scientists are working avidly to find ways to minimize side effects.
Houston-based Bellicum Pharmaceuticals, for instance, is designing two switches to help control the deployment of T cells.
One is triggered by a drug called Rimiducid, which turns on a “suicide switch’’ in the T cell, causing it to die. The second works more like a gas pedal that can control how fast the cells proliferate in the body and attack the tumors, Bellicum CEO Tom Farrell said.
The goal: to be able to control the patient’s response and to minimize side effects.
Bringing CAR-T to the mainstream
To learn more about CAR-T, doctors say it must be used more broadly.
“If we can get cellular therapy out of academic institutions, and out into mainstream medicine, we’ll have more understanding of its power,’’ said Goff, the National Cancer Institute surgeon.
But that’s tricky because of the side effects. Education is critical: When any company rolls out a new therapeutic, part of its duty is to teach physicians how to appropriately use the product. This is exceptionally important with CAR-T therapy, said Dr. David Chang, chief medical officer of Kite Pharma.
“I don’t want to sugarcoat the adverse events for CAR-T therapies,’’ Chang said.
However, he said, CAR-T is meant to be a one-time therapy. After an intense burst of treatment, patients ideally recover from their cancers and go on to lead relatively normal lives.
This “really is moving away from the paradigm of repeat chronic treatment we’ve become accustomed to in oncology,’’ he said — so he thinks with training, it could someday become fairly routine in hospitals across the country.
Others aren’t so sure, at least not yet. “Whether this will be technology that’s specific to boutique, high-end academic centers, or technology that can be used in community hospitals if people learn how to infuse them in a safe manner — we just don’t know yet,’’ said Dr. Renier Brentjens, director of cellular therapeutics at Memorial Sloan Kettering, who is working with Juno on its CAR-T treatment.
As for Koehler, these days she feels good — for the most part.
Her energy levels are better than they were before the CAR-T therapy, and the cancer-free diagnosis has kept her spirits aloft. But she needs regular infusions of immunity-boosting drugs, because her new T cells are still killing off other immune cells. Koehler can’t work, and she still gets sick very easily.
Despite the agonizing side effects, she says she’d do it all again.
“When we realized I had a nuclear bomb in my body, we were very scared,’’ she said, “and when we learned that I was cancer-free, all I could think was, ‘How blessed am I?’’’
Meghana Keshavan can be reached at Meghana.Keshavan@statnews.com. Follow her on Twitter @megkesh.